Home / Treatments / Undescended Testis

When the baby is formed in the womb, the testis is initially formed at the back of the abdomen (tummy). It then slowly descends down to the bottom of the abdomen, into the groin and finally through the inguinal canal to reach the scrotum (sac of testis). Most baby boys are born with testes in the scrotum. If the testis has not completed the descent then it is called an undescended testis (UDT).
At birth about 5% of boys have an undescended testis. In two-thirds of these boys the testis comes down to the normal position on its own by 3 months of age. After 3 months it is unlikely to descend on its own. The overall rate after the age of 1 year is about 1-2%. About 10% of UDT are bilateral (both sides).
In some boys, especially between the age of 1-7 years, the testis intermittently pulls up from the scrotum into the groin. This is due to a very active muscle in the spermatic cord (cremasteric reflex). Usually a warm bath relaxes the muscle and the testis comes down. This condition requires no treatment. However, some retractile testes can later become true undescended testes (ascending testis) and require surgery.
An undescended testis that is left untreated carries the following risks:
If the testis has not descended by 6 months of age, it is unlikely to come down on its own. Surgery is recommended between 6 months and 1 year of age. Early surgery gives the best chance for the testis to develop normally and produce sperm.
There is no role for hormone treatment (HCG injections) in true undescended testis. Hormones may help in some cases of retractile testis but the evidence is not strong.
The operation is called orchidopexy. If the testis can be felt in the groin (palpable), a small cut is made in the groin crease. The testis is freed from surrounding tissues, the associated hernia sac is dealt with, and the testis is brought down and fixed in a small pouch created in the scrotum.
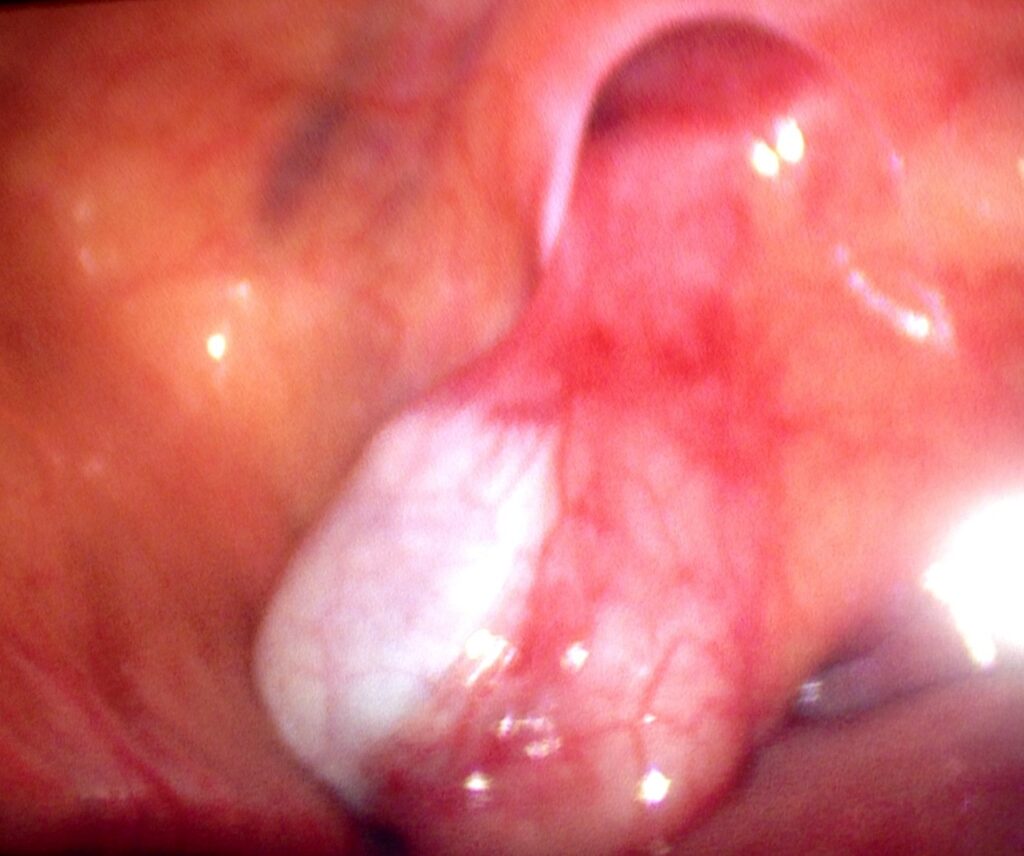
If the testis cannot be felt (impalpable / non-palpable), laparoscopy (keyhole surgery) is performed first to locate the testis. About 50% of impalpable testes are found inside the abdomen. A staged operation (Fowler-Stephens) may be needed to bring a high abdominal testis down to the scrotum.
In about 20% of non-palpable undescended testes, the testis has vanished due to a twist in blood supply before birth (vanishing testis or testicular regression). Laparoscopy confirms the absence. A testicular prosthesis (artificial testis) can be inserted at a later age for cosmetic purposes.
Orchidopexy for a palpable undescended testis has a success rate of over 95%. For impalpable testes requiring laparoscopic surgery, the success rate is around 85-90%. Early surgery (before 1 year of age) gives the best outcomes for testicular growth and future fertility.